Clavicle Plating System: Midshaft and Distal Clavicle Bone Model
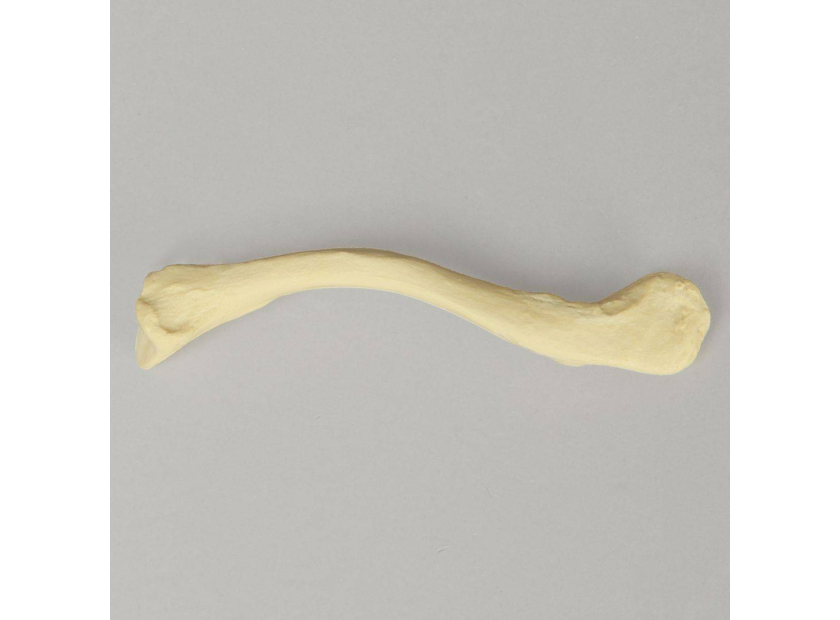
Clavicle fractures are quite common, making up about 5% of all adult fractures. A clavicle plating system allows for early patient mobilization after fracture reduction. Anatomical midshaft and distal clavicle bone models are effective at facilitating hands-on learning when training with a clavicle plating system. Let's take a closer look.
Clavicle Plating System
A clavicle fracture often results from a fall that exerts enough pressure to break the collarbone. While many clavicle fractures can be immobilized with a sling, some fractures require surgery to realign the collarbone.
Clavicle plating systems are designed to treat simple and complex breaks in the collarbone as well as malunions and non-unions. Clavicle plates are titanium plates used to stabilize and fixate the collarbone after fractures have been accordingly reduced.
Different clavicle plates are designed to treat various fractures:
- Distal clavicle plates: Support healing of coracoclavicular (CC) ligament as well as injuries near the acromioclavicular (AC) joint
- Midshaft clavicle plates: Support healing of injuries to the periosteum
- Anterior clavicle plates: Support healing of injuries to the periosteum
- Clavicle hook plates: Designed to avoid or minimize contact with rotator cuff and nearby soft tissue when treating distal clavicle fractures
Clavicle plating systems enable safe mobilization by providing absolute or relative stability as required by the treatment. Plate design is generally aimed at the preservation of blood supply to the fracture area while restoring the correct anatomical relationship.
Hands-On Training with Anatomical Models
Given the shoulder's tight spaces, training with anatomical models helps residents and medical representatives master the clavicle plating system thoroughly before they even enter an operating room.
|
Plate Selection |
Bone models are excellent at facilitating instruction and demonstration when it comes to the proper selection of clavicle plates. Factors for selection, including variations in patient anatomy and the nature of the fracture, can be discussed. Some clavicle plating systems come with a plate sizer that may be used on anatomical models to familiarize trainees. Distal clavicle bone models also demonstrate how clavicle hook plates protect the rotator cuff or enable fixation in cases where there are not enough distal bone fragments for proper fixation. |
|
Plate Bending |
Instructors may select one or more anatomical models to show how plates can be manipulated using irons and pliers to contour them to different bone lengths. Discussion can also center on best practices, such as making a series of small bends, avoiding over-contouring, and keeping the integrity of the plate intact. Midshaft clavicle models may be used to assess the conformity of the contoured plates to the selected bone length. |
|
Plate Insertion |
(Instructors may demonstrate reduction techniques on models beforehand as necessary.) Residents and medical representative trainees may practice plate insertion on midshaft and distal clavicle models designed for cutting and drilling. Manipulation of clavicle plating system instruments such as forceps, reduction devices, hexalobe drivers, and drills may be practiced as well during plate insertion. Best practices such as avoiding the subclavian neurovascular bundle and applying gentle force when drilling may be emphasized. |
|
Screw Insertion |
Instructors can show how screws should be placed to fixate major fragments of a fracture. Placement of an interfragmentary screw may also be demonstrated to reinforce fixation. The use of a gauge to determine the length of each screw may be practiced on foam models. Instructors can use distal and midshaft clavicle models to show how neurovascular structures may be protected from overdrilling with the use of a retractor. Insertion of locking screws may be practiced on conducive models. Best practices, such as the use of K-wire to verify final screw placement, avoiding contact with the subclavian artery and brachial plexus when drilling, and avoiding excessive torque, may be discussed. |
|
Plate Removal |
Residents and medical representative trainees may practice implant removal on midshaft and distal clavicle models. Hook plate removal from distal clavicle bone models can also be practiced, as it requires a different procedure from typical clavicle plates. The use of alternative instruments and techniques in the case of stuck screws may be discussed. For example, a slight angling of the driver, along with the gentle application of a mallet, is an effective way to loosen resistance. Best practices, such as unlocking all screws before removing to avoid plate rotation, can be emphasized during instruction. |
In summary, anatomical models allow residents and medical representatives in training to explore a clavicle plating system through hands-on exercises. Residents can practice fixation procedures, such as cutting, drilling, and screw insertion, on midshaft and distal clavicle models. Anatomical models also facilitate the assessment of plate bending and manipulation to ensure the desired fit with various bone lengths. Lastly, anatomical models help residents and medical representative trainees practice implant removal using a clavicle plating system.
Best-in-Class Models For Clavicle Plating System Training
Sawbones designs and manufactures best-in-class anatomical models for residents, instructors, students, sales specialists, and more. We offer a wide variety of clavicle bone models for medical training and display purposes including:
 |
|
|
Clavicle with Transverse Fracture, Solid Foam
|
Clavicle with Scribed Fracture Line, Solid Clear Plastic
|


Sawbones is a proud partner of several medical training institutions, including the Medical Sales College.
Sawbones offers the best-in-class anatomical models for clavicle plating system training and demonstration. For more information on our offerings or to talk about custom training models, contact us at 206-463-5551

Work with the industry leader in medical training products!
For four decades, Sawbones has offered the best medical training products for doctors, educators, sales specialists and more. Contact us to learn more about our high-quality models!
1 (206) 463-5551Contact Us!